
Categories
Blogs & Podcasts
Atheism
Atheism, in its most direct definition, is the absence of belief in gods or deities. It does not constitute a…

The heartbreaking death of 7-month-old Elizah Turner in Columbus, Ohio, on April 9, 2025, serves as a grim reminder of…

Categories
Blogs & Podcasts
Fate and Karma
When we think about why things happen in life, two concepts often come up: fate and karma. These terms are…

Alejandro Jodorowsky’s poignant metaphor, “Birds born in cages think flying is an illness,” encapsulates a profound truth about human perception,…

Diamonds have long been symbols of luxury, romance, and enduring value. However, beneath their glittering facade lies a complex web…
Categories
Discourses
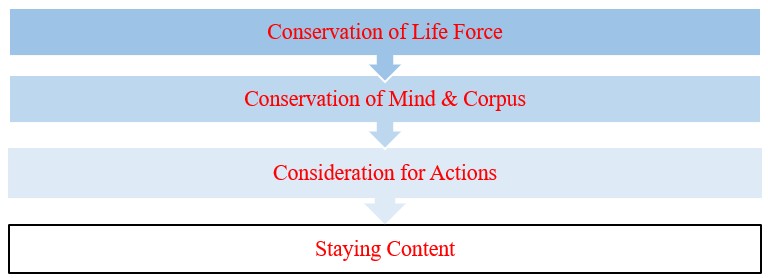
Core Values for Humanity
Shree Agyatananda has studied several ancient texts & treaties, to present us with the concept of most important values for…

Categories
Blogs & Podcasts
Karma of the Humanity
INTRODUCTION TO THE COLLECTIVE KARMA OF HUMANITY We discussed the karma earlier. In that post, we had discussed the existence…

Categories
Blogs & Podcasts
What is Karma?
INTRODUCTION Most of us have heard a proverb in English. It says “as you sow, so you reap”. Almost all…